A 55 years obese patient admitted in emergency department of DMCH with the C/O breathlessness, pain abdomen, irritability. She was taking corticosteroid for longer period and had moon facie, obesity, hypertension and pateche. Before ABG she was give O2 inhalation 5 L/min, Diuretics, corticosteroid, nebulisation, Inhalation with salbair I. iv fluid, pantoprazole, antibiotics without improvement. Then after 48 hrs patient was transferred to ICU and ABG was done.
ABG Analysis
1. Gas Analysis
Step: 1
Pao2 = 135.3 mm of Hg – Above normal, due to high Fio2.
Step:2
PAo2 = 135.3 mm of Hg – Above normal, due to high Fio2.
Step: 3
P(A-a)o2 = (135.3-135.3)
= 0, below normal – no Parenchymal lung
disease.
Step: 4
PaCo2 = 15.7 mm of Hg – low – Hyperventilation.
No, respiratory failure.
Step: 5
Patient has below normal PaCo2 with no increase in
P(A-a)o2 and The Fio2 is not less, so no respiratory
cause of increased respiration.
Step: 6
P/F = 135.3/40X100 (Here Fio2 = 50%)
= 338.25 No ALI
Step: 7
The relation between Spo2 and Pao2 are normal.
Step: 8
Cao2 = 5.5X10X1.34X99/100+0.003X135.3
= 5.5X1.34X0.99+0.003X135.3
= 72.963+0.4059
= 73.369
The weight of the patients is 65 kg.
So expected normal Cao2 in this patient = 180.6 ml of O2/L
But it is = 73.369
So it is one cause of dyspnoea.
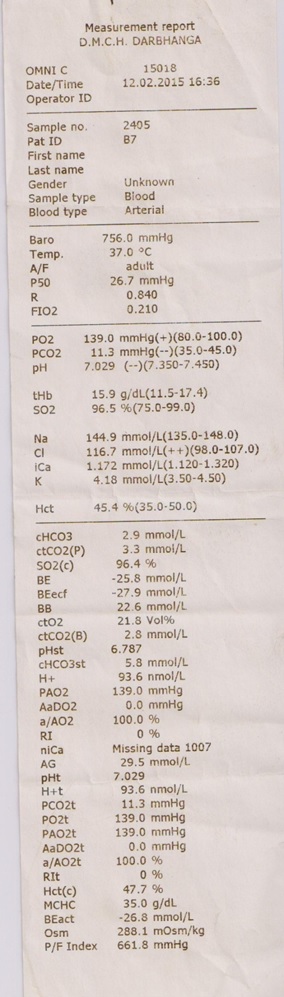
2. Electrolyte Analysis

Ca++ – 0.166 mmol/L – Low -> Cause of Hypocalcaemia is needed to be
searched.
K+ – 1.25 mmol/L – Low -> i.e. losses in gastrointinal or renal cause
here probably due to diuretic use.
Anion Gap :-
26.4 mmol/L -> So AG>20 mmol/L
Support a primary metabolic acid base disturbance.
Delta Gap :-
Delta Gap = 26.4-12
= 14.4
Delta gap + HCo3 = 14.4 + 10.5
= 24.9 falls in between 22-26 mmol/L, Normal
So no metabolic alkalosis and no non-anion gap metabolic acidosis.
Gap – Gap Ratio :-
Gap-Gap ratio = (26.4-12)/(24-10.5)
= 14.4/14.5 =approx 1
Indication high AG metabolic acidosis.
Base Excess :-
Base Excess (BE) = -12.5 -> Metabolic acidosis.
It also justified.
3. Acid – Base Analysis
Step: 1

Step: 2
HCo3 = 10.5 mmol/L -> metabolic acidosis .
Step: 3
PaCo2 = 15.7 mm of Hg (< 40 mm of Hg) so, respiratory alkalosis.
Step: 4

H+ & HCo3– move in same direction.
So, respiratory cause. So, Respiratory Alkalosis.
Step: 5
So, PaCo2 & HCo3– move in same direction.
So, simple cause (fallacy of the formula, because there is metabolic acidosis confirmed).
So, other way to know about mixed disorder is to evaluate.
Expected value of PaCo2 = 46
Actual value of PaCo2 = 15.7
So, Expected value and actual value of PaCo2 do not match -> So, mixed disorder present.
So, High Anion gap Metabolic acidosis with Respiratory alkalosis.
Step: 6
Compensatory change
Predicted comparative of PaCo2 fall = 1.2 X (24-10.5)
= 1.2 X 13.5 = 16.20
So, Expected value of PaCo2 = 40 – 16.20 = 23.80
The value of PaCo2 is 15.7
Much less than 23 – 80
So, Respiratory Alkalosis associated.
Final diagnosis
The patient has mixed disorder of high anion gap metabolic acidosis with respiratory alkalosis
with dehydration with hypokalaemia with hypocalcaemia without ALI/ Parenchymal lung disease.
Causes of Respiratory Alkalosis
L – Liver disease – Increase SGPT
E – Embolism – Not
D – Drug
A – Anxiety – Present
V – Ventilator – Not
P – Pregnancy – Not
H – Hyperventilation – Present
Causes of High Anion gap metabolic acidosis
M – Methanol – No history in this patient
U – Uraemia – Not present
D – Diabetes mellitus – Not present
P – Paraldehyde – No history
I – Infection (CBC) Present , Ischaemia (ECG) Not Present
L – S.lactate – Not done
E – Ethanol – No history
S – Starvation, Salicylate



 H+ & HCo3– move in same direction. so, respiratory cause.
H+ & HCo3– move in same direction. so, respiratory cause.